hierarchy of evidence
Cohort studies? Case series? Anecdotal? Eh?!?
You’ll have seen “scientific and clinical studies or evidence-based” used quite a bit across our website, so we thought we’d take some time to teach you about the different levels and types.
So here we go…
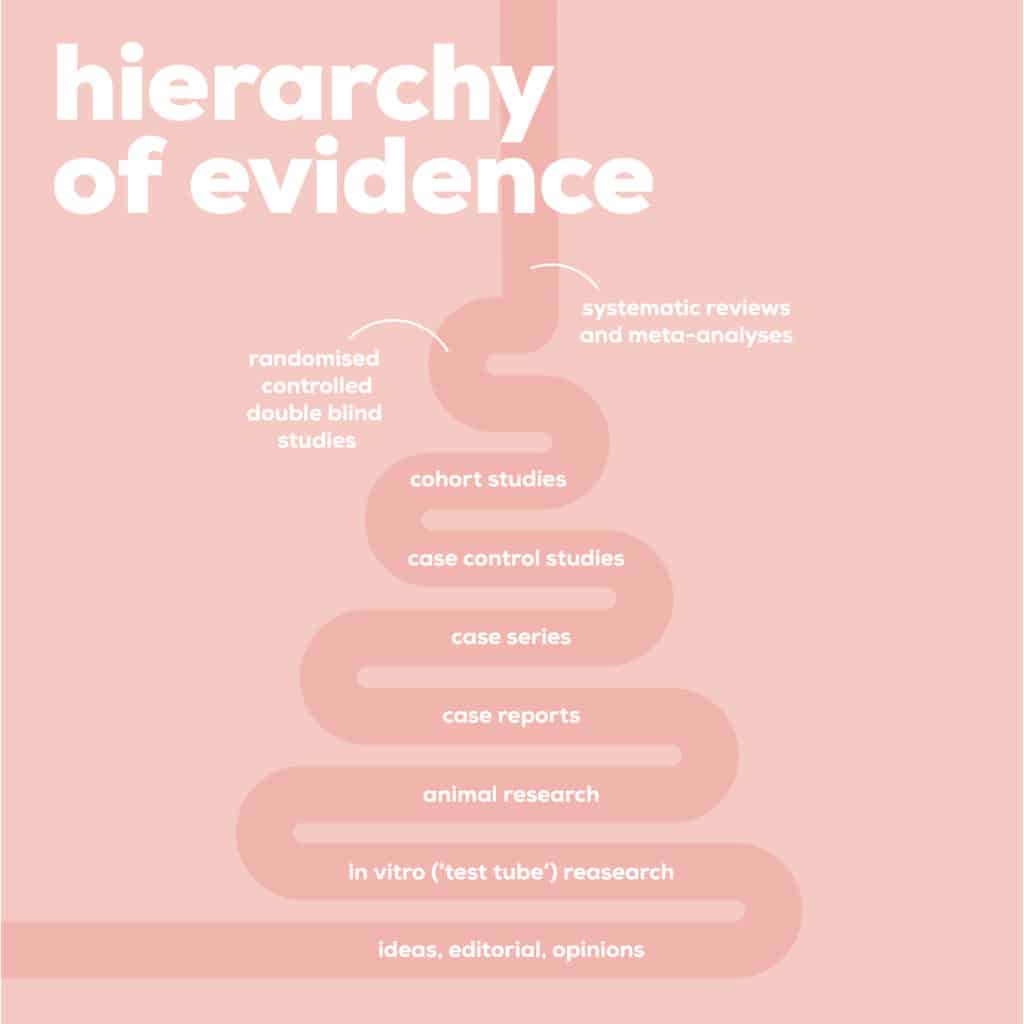
The ‘hierarchy of evidence’ is basically a league table for different types of scientific research.
Systematic reviews are in poll position followed shortly after by RCTs, which actually stand for Randomised Controlled Trials, coming in at no.2.
Systematic reviews pool all the relevant studies on a topic (for example, the effect of probiotics on IBS symptoms) and try and reach a general conclusion based on all the studies available. Because no single study counts as definitive proof, it’s always important to have a view of the bigger picture before coming to a conclusion, which is why systematic reviews are top dog. While bias is minimised in a systematic review, caution and a degree of critical thinking is still needed – in a systematic review, it may look at several small studies and pool them together which would amplify any positive findings and magnify potential negatives. This can result in a misleading conclusion about a particular area.
What we love about them is the easy to read summary that normally hides at the back (so don’t feel you need to be a statistician to understand the outcome). But when we talk about the individual studies reviewed within these systematic reviews, RCTs are widely considered the most reliable type of single study you can do BUT they too can have flaws…more on this later.
Why is that then?
Not only are RCTs therefore good for monitoring what happens when you make people do something very specific, very differently, but they also RANDOMLY allocate participants to different groups for testing within the trial (intervention or no intervention). This reduces the potential bias that may arise when selecting individuals for different groups. There are quite a few variables within this randomisation and this all affects the reliability of the results.
For example, do the participants know what they are receiving? The placebo effect is a real thing! That’s why you will see single-blind (participants didn’t know) or double-blind (neither the researchers or participants know) when it comes to the intervention. If the study is not blinded, there is a question whether researchers assigned study participants into different groups based on how ill or well they thought they were.
The participants are then followed up on after a set period of time, with the theory being that as the groups should be the same (on average), any differences between the groups will be due to the intervention (in theory…).
When looking at a RCT, always check out who it has been funded by (e.g. a pharmaceutical company), the study size and blinding. These are just a few things you need to watch out for with RCTs to make sure they’re as reliable as can be.
Why are RCT’s so important? Well, they’re often called interventions, as they’re unusual, as scientists actually DO something to study participants and then look at what happens once they have (e.g. a supplement or mindfulness). Other types of research design may involve a laboratory experiment in controlled surroundings (so not real life) or use surveys to observe people ‘in the wild’ and then try and draw links and conclusions between different treatments or risk factors and their outcomes.
Hopefully this will make it all a bit easier to decipher and help you apply a critical eye to reviewing the evidence!